Often we are faced with a health challenge that we seek out care for and in return get multiple differences of opinion. Sometimes a family member may push us one way or the other based on their personal life experience. Other times it may be a friend in the medical field that guides us to a specific specialist to help steer the ship in the right direction towards a potential remedy. Unsure of what exact treatment is needed, we try to make the best decision with all of the collected information and hope and pray that it will have a positive impact on treating the condition.
When treating scoliosis there are multiple approaches to go about it and I, the writer, will not be recommending one. This is due to the fact that I never went to medical school and have never treated a patient with scoliosis. I leave that up to licensed orthopedics, surgeons, and doctors. However, I would like to lay out what a caregiver may hear when searching for a scoliosis treatment regimen in order that when riding atop the ship of scoliosis treatment options, you have just a little clarity and are able to make a more educated decision.
Why Can’t Scoliosis Just Heal Itself?
Assuming that the scoliosis is significant enough that you are reading this article, you need to know that it will not simply correct itself. Every healthy human being has some spinal asymmetry that gives a slight curve to a healthy spine. We were made that way in order for us to be more flexible allowing us to be mobile with proper spinal support. The problem arises when there is a curve of +10° which means that the individual has a condition referred to as scoliosis. Anything less than 10° would be still considered normal and not require treatment.
When the spinal asymmetry has a curve of greater than 10° there is a fundamental problem with how the spine is supporting the body. Keep in mind that the spine is the central support structure for the body’s musculoskeletal system. When the spine begins to curve beyond the normal limit it impacts the whole entire body. This might mean one leg is longer than the next or that hips or shoulders are leaning to one side. Besides the pain that is present in people with scoliosis there is a major social element of looking different. Clothes don’t fit the same, pool parties are avoided, and patients begin to have the perception that everyone is looking at them.
The spine will not revert back to a normal curve unless it is treated. It’s like a building built on a slight angle, that all the weight is leaning to one side rather than being distributed evenly. Scoliosis is the same way and when the weight is leaning to one side those bones and muscles are more strained which can result in pain. Leaving it won’t change anything especially if the spine is not fully developed as would be in the case of a young girl or boy. As a matter of fact, the curve could worsen and make it more difficult for them to do the basic activities kids love to do like playing sports. Finding the right treatment regimen may take some time but it must be addressed for the child’s well being.
Are All Scoliosis The Same?
Not all scoliosis is the same. Some are flexible and not rigid while others are structural with rigid curves. Flexing out the scoliosis when the curve is set structurally won’t really do much. Pulling on the spine will not correct a person’s scoliosis because that is the makeup of the patient. It’s almost like trying to straighten out a warped piece of wood. If you do get it to straighten out with force it will revert to its original curve with little to no impact and change to its shape. Often chiropractors will implement a treatment regimen which includes laying the patient down on a therapy table and pulling their head while keeping the body in place. In theory what is supposed to happen is that the spine is supposed to get flexed and begin to straighten itself out. However, the makeup of the spine is to flex, rotate, and absorb impacts. This can include jumping, falling, or getting tackled in a football game. With each impact the spine will naturally flex in different ways to protect itself and the body it supports. Having a chiropractor pull on it might feel good but chances are that it will have little to no impact on treating the scoliosis.
When Is It Necessary To Have Surgery To Treat Scoliosis?
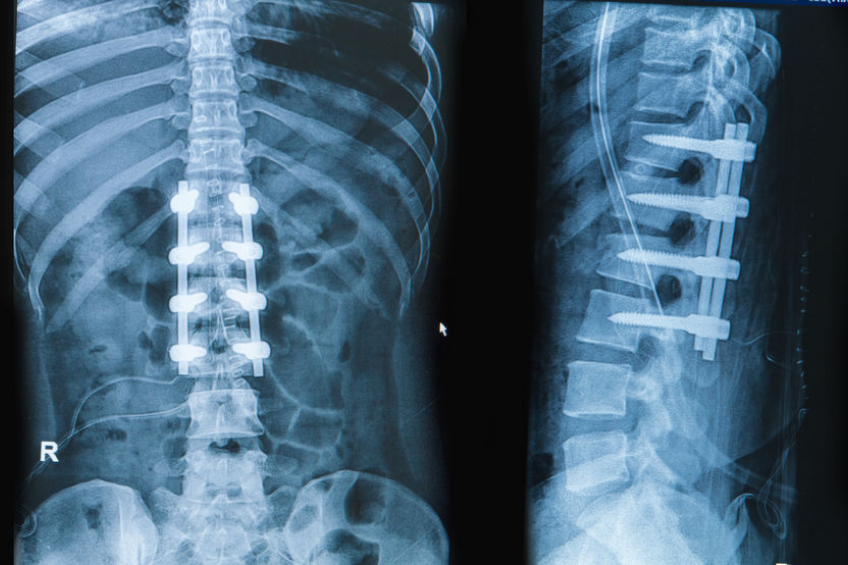
According to the American Academy of Orthopedic Surgeons most scoliosis surgeons will agree that when there is a spinal curvature between 45° to 50° or higher surgery would be required to lessen the curve. Surgery will realign the vertebrae in the spine by fusing them together and create a more normal spinal asymmetry. The recovery for such a surgery is usually three to six months but the way each patient takes to the surgery may be different. In the end of the day it’s surgery and the body undergoes significant trauma to get back to itself. Many young athletes that have scoliosis will opt in for such a surgery as they are looking for a quick fix in order that they get back to a sports program. However, patients and caregivers need to know that not always does surgery fix the problem. The objective is to fix the curvature of the spine which should result in less pain and a better quality of life but not always that is the case. Surgery needs to be taken seriously and patients who go through surgery need to hope for the best and give themselves proper time to heal prior to getting back into a normal routine.
Treating Scoliosis Through Bracing Therapy
Before opting in for scoliosis surgery it would be worth your while if you spend some time researching if scoliosis therapy is right for you. The good part about it is that it is non-invasive and won’t require a long recovery time. However, it will require the patient to be fitted with a brace that will help realign the spinal structure. The brace will be worn around the clock until the therapy is complete and the spine reverts back to a normal curve.

Bracing is not a new orthopedic device that is used to help treat scoliosis. In fact, the first scoliosis brace was created by a French army surgeon by the name of Ambrose Paré in the 1500’s. He developed supportive braces that were used to treat spinal deformities for soldiers in the French army. The method of treatment was to use pressure from the braces to reduce the dislocation of the spinal asymmetry.
Over the course of time bracing for scoliosis became more prevalent and the Milwaukee Brace, Wilmington Brace, and the Boston Brace were introduced to patients through the twentieth century. Each had their pros and cons but were rather bulky and hard for patients to wear for the 23 hour a day brace treatment regimen. With time brace creators had begun to make the brace sleeker, lighter, and perfectly formatted for the patient that helped making wearing the brace easier throughout treatment. In 1970, Dr. Jacques Cheneau of France and Dr. Emanuel Rigo of Barcelona, Spain introduced the Rigo-Chêneau Brace. This brace was designed according to each patient’s specific pressure points and allows many breathing points for comfort. The duo of a highly effective brace while keeping the patient comfortable would make it easier for an effective and shortened treatment plan for scoliosis. Bracing might not be for everyone but it’s worth discussing with your pediatrician to see if it might be an effective way to help treat your boy or girl’s scoliosis.
Final Words
Seventy to eighty percent of scoliosis is referred to as “idiopathic scoliosis” which means that there is no common cause for the scoliosis. There are other types of scoliosis which we do know the cause of like neuromuscular scoliosis, degenerative scoliosis, adolescent idiopathic scoliosis, and congenital scoliosis. When a child has a spinal curve of 10° or higher it needs to be addressed and monitored to make sure if it does not worsen. Always ask the patient how they feel because scoliosis can sometimes be painful and make it difficult to treat. If the patient is treated with bracing therapy it may be difficult at first to get used to wearing the brace but keep in mind that it won’t be forever. As per the Rigo-Chêneau Brace most patients will get used to it within a week and can complete the therapy in about 12 to 16 months.

If there is a significant curve in the spine of greater than 50° surgery might be the only option. Caregivers need to know that living with scoliosis is painful and it will not change by itself unless it gets treated. The spinal structure needs to be attended to and until then your loved one will be living in pain and that’s quite unfortunate. Be smart and get it checked out while it can be treated. Once the spinal growth is complete it’s much more challenging to straighten out the spine.