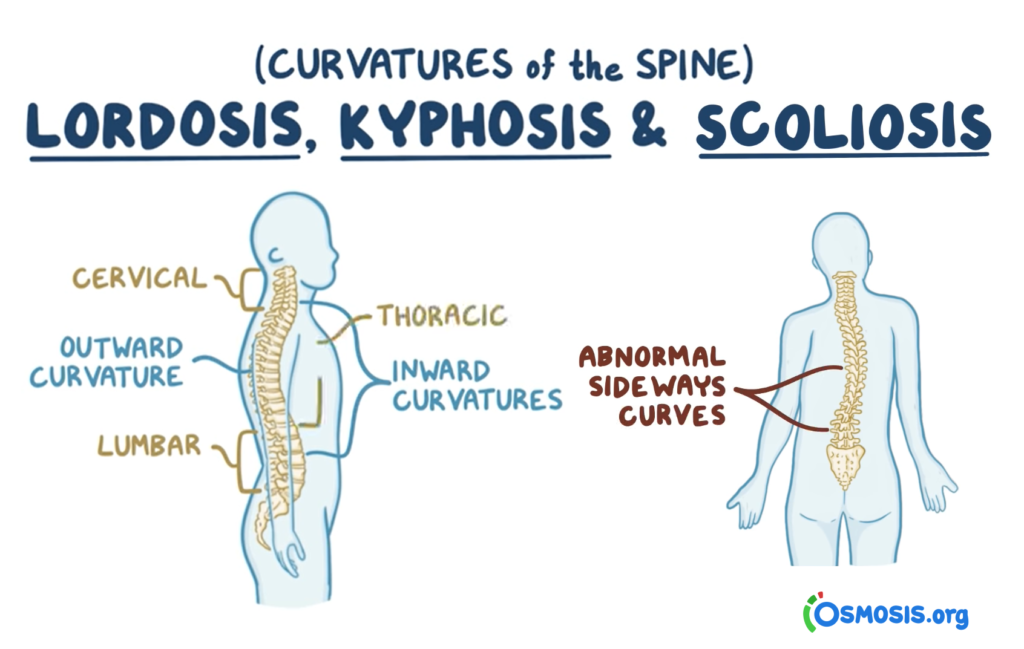
“Scoliosis! Oh, no, not again”, exclaimed a quite upset mother named, Katie. Katie had just finished a well checkup at her pediatrician with her eleven-year-old daughter, Marla. One of the reasons Katie trusted this doctor was because he was an expert on childhood scoliosis. Katie has four children, one boy and three girls. Her oldest daughter, who is married now, had to be treated with a brace for scoliosis as a teenager. Her other two children were free of this spine disorder, so she was surprised and disturbed when her doctor proclaimed that Marla had a twenty percent curvature of the spine.
Katie has been quite diligent trying to prevent her children from developing scoliosis since her oldest child’s diagnosis. She made sure that her babies slept on a firm mattress trying not to take them with her to bed. She researched the best highchairs and carriages that would keep her babies’ backs taut and straight. She also performed exercises with her babies to prevent flat head syndrome and torticollis. By switching the sides of the crib and positions of sleep of her babies, keeping them on their tummies, and playing with them instead of keeping them on their backs, she was successful in avoiding the symptoms of early bad posture.

At twenty percent, most doctors will prescribe the watch and wait method, however, Katie would have none of that. She immediately made an appointment with her neighborhood scoliosis center and was able to start Marla on physical therapy and hopefully she will avoid brace therapy.
Usually, scoliosis therapy is started at about a 25% Cobb curvature measurement. Increasingly, doctors and parents are becoming aware that there is a genetic factor associated with childhood scoliosis. Recent research studies are showing that there are genes, enzymes, neurotransmitters and hormones (a reason why the incidence of scoliosis is more prevalent in girls) that are responsible for scoliosis. Postural memory is the term used when the patterns of the brain are altered causing abnormal production of hormones, key proteins and nervous system problems.
These are some of terminologies we will examine in this article, zebrafish, manganese, SLC39A8, ladybird homeobox gene, LBX1, and CHD7.
Manganese
Let’s start with the simplest slightly familiar sounding term, manganese. Manganese is a type of mineral found in whole grains, nuts, seeds, legumes, tea and leafy green vegetables. It is considered an essential nutrient for the human body to function efficiently. There is a type of medicine taken by mouth for manganese deficiency.
Manganese is both good and bad. It can be an essential mineral and a toxin. High doses of this mineral can cause tremors, walking difficulties and psychological symptoms such as hallucinations and personality disorders. Manganese deficiency in animal studies can impair growth and cause curvature of the spine.
In humans, the gene does not stop working totally, but rather it does not working optimally. It seems easy enough to just supplement the diet of the child who suffers from severe scoliosis with manganese, but it is not that simple. Scientists at Washington University (published in the journal, Nature Communication), have found that children with severe scoliosis are two times as likely than children without this spinal disorder, to carry a gene that makes it hard for their cells to take it in and use manganese.
Professor Christina Gurnett scanned all the genes of 457 children with severe scoliosis and 987 children without severe scoliosis. The gene, SLC39A8, was present in only six percent of the unaffected children but present in twelve percent of the children with severe scoliosis.
A separate research group took 1,095 unaffected children and tested them against 841 affected children with moderate to severe scoliosis and found that the children with scoliosis were twice as likely to carry the gene. The study found that those with the gene could absorb zinc and iron but not manganese. Blood tests on the children with the gene revealed lower levels of manganese.
There is a test on the market, called ScoliSMART which costs $299. This test can identify specific genes (or SNPs) that are associated with idiopathic scoliosis. This test helps the doctor assess the best course of action to minimize the effect of these genes on spine curvature and stop it from worsening. The test can pinpoint genetic disposition for developing scoliosis in children before diagnosing actual spine curvature. “ScoliSMART labs, have discovered twenty eight genomic functional variant groups directly associated with idiopathic scoliosis” (according to Dr. Clayton J. Stitzel) If this test is indeed as effective as the company claims, it could have been used by Marla’s doctor in our introductory story.
Ladybird homeobox 1 (LBX1)
A genetic chain reaction due to ladybird homeobox 1, an overactive gene, is found to be the start of a genetic chain reaction causing the spine to grow abnormally according to Asian Scientist (April 19, 2016). These findings were also published in PLOS Genetics.
Several types of genetic experiments on a small freshwater fish called the zebrafish, were performed in research labs to mimic scoliosis. By manipulating the genes of the zebrafish with an excessive amount of the gene, LBX1, scientists were able to monitor how the spines of these fish developed. Timing of when too much LBX1 is injected into the fish was crucial in the way the fish bodies developed.
1) When embryos of the fish were injected with extra LBX1, the cells of the backbone and back muscles were seen to be wider than in healthy fish. The fish that survived the experiments developed misshapen bones in their backs on which scoliosis could be observed. Researchers were excited because the experiment with the zebrafish models the defect of scoliosis in humans with the same misshapen bones in a smaller version.
2) In a modified experiment, the zebrafish were injected with extra LBX1 throughout their lives. The gene was only injected into some cells called research genetic mosaics. Interestingly some of the fish bones were correctly shaped but their spines grew curved as they entered adulthood. This experiment was very important since it is typical for most human cases of scoliosis, where initially there are no signs of back problems until the time of growth spurts just before and during adolescence. Adolescent scoliosis affects two to four percent of all children ages ten to sixteen.
The female zebrafish were noticed to develop scoliosis more than the male fish. As noted earlier, adolescent- onset scoliosis is more prevalent in girls and as of yet researchers are not accurately giving reasons although female hormones are noted by some to be one of the causes. Osteoporosis in adults is more prevalent in women for the same hormonal reasons.
Hormones
There is strong evidence that scoliosis is family related. Almost one third of the patients with adolescent idiopathic scoliosis have a family history of this condition as Marla in our introductory story. First-degree relatives have an eleven percent chance of also having this problem.
One of the studies indicated that only nine percent of the boys and twenty-nine percent of the girls whose parent had scoliosis developed it as well. This indicates a strong likelihood that the hormone, estrogen may be the cause. The study suggests that specific genetic variants can cause “estrogen signaling dysfunction”. When a female patient who has this type of a gene, enters pre-teen growth spurts, excessive estrogen will be produced causing scoliosis.
CHD7 Gene
Dr. Carol Wise, at Scottish Rite Hospital, assembled data on fifty-two families with a history of scoliosis. One family member was from an earlier generation and the other family member was there for treatment. They scanned the patients who had an average curvature of forty degrees and were otherwise healthy. CHD7 is a protein that is crucial in the development of a healthy and straight spine. The researchers theorized that although the production of this protein was not actually disrupted, the gene mutation alters the binding of a molecule preventing the actual gene from turning on correctly. Then the amount of CHD7 that is produced decreases.
According to Dr. Michael Lovett (professor of genetics and pediatrics) the linking of the gradual worsening of scoliosis with the slow decrease in the production of CHD7 protein means that just the same way that scoliosis develops slowly over a long period of time, so too the protein decreases slowly over a long period of time.

Fascinating advances are being made in finding the genetic causes of adolescent scoliosis. Genetic testing in general is quite controversial especially in religious circles. Testing singles before marriage to see if they are carriers of genetic diseases is encouraged in certain communities.
Carrying this idea to an extreme would be worrisome and unnecessary, if there is not much that can be done to prevent certain diseases (for example, certain dispositions to certain cancers). However, testing for scoliosis if it runs in the family, could be quite beneficial and not problematic.
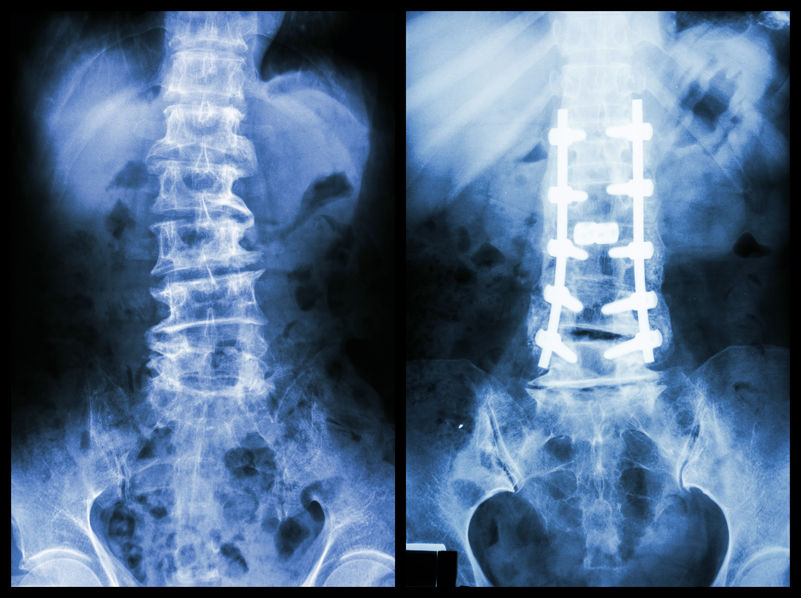
Using these new gene tests appropriately, and with the doctor and parent being on the lookout for subtle changes as the child gets close to puberty, could prevent major therapies and surgery. Instead, the child could be seen by a physical therapist at their local scoliosis center and be treated with either exercises or brace therapy before the curvature becomes more severe.