
Understanding Bracing Effectiveness When Treating Adolescent Idiopathic Scoliosis
There are many white papers that discuss the effectiveness of various therapies for treating adolescent idiopathic scoliosis (AIS) but few are brought down to a comprehensive level for parents. Years of research are done along with the aggregation of highly credible data from prominent medical journals. But what does n = 56 + 63 + 102 + 34 + 80 mean to a mother looking for treatment options for her daughter’s scoliosis?

The objective of the content below is to extract the main information from a white paper titled “The Effectiveness of Different Concepts of Bracing in Adolescent Idiopathic Scoliosis (AIS): A Systematic Review and Meta-Analysis” done by the Journal of Clinical Medicine and make it comprehensive to any parent whose child is suffering from scoliosis. The white paper was published by the Journal of Clinical Medicine on May 15, 2021, making it very relevant to patients with adolescent idiopathic scoliosis.
Basic Definitions To Makes Sense Of Study On Scoliosis Bracing Therapy
Prior to delving into the actual study and findings, it’s important to define certain terms that will be used in the white paper. Most of the words that will be used are related to the spinal skeletal maturity of the pelvic area of the patient. Readers should be cognizant that the spine rests directly on top of the sacrum bone which is supported by the pelvis.
Ossification: This is the abnormal bone formation generally referring to soft tissues becoming calcified and hardened. Often soft tissue can become hardened through the conversion into calcium which is referred to as “calcified”. For laymen such as us it means a soft area by the bone becoming hard.
Iliac Apophysis: When this term is being used it’s referring to an inflammation around the tendon areas situated near the front of the pelvis. The inflammation could be caused by injury but in our case it’s the irregular growth of the child that causes it. For us layman such as us it means inflammation of the tendons in the front pelvic area.
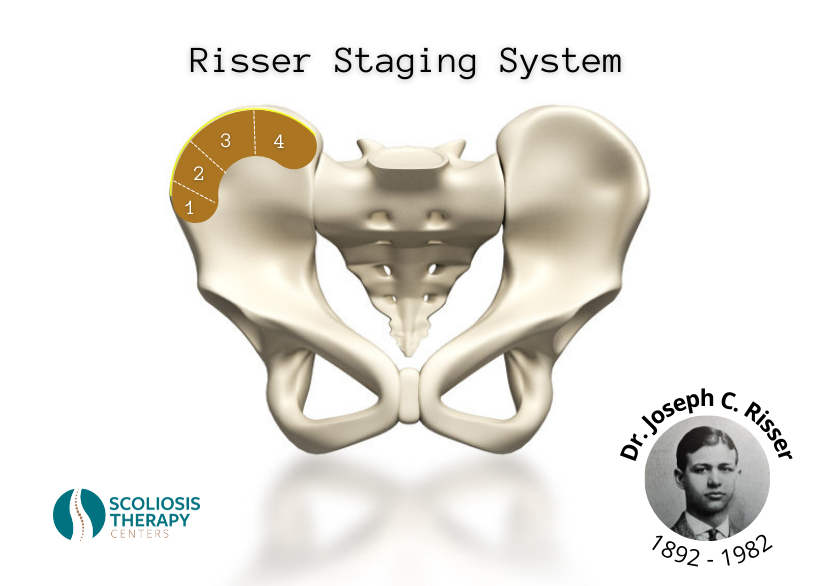
The Risser Staging System: Dr. Joseph C. Risser (1892 – 1982) was someone who was monumental in treating scoliosis. Risser recognized that the abnormal bone formation and tendon inflammation of the pelvic area (ossification of the iliac apophysis) had very much to do with the patient’s spinal skeletal maturity. In 1958 his many years of research was recognized and clinicians had begun to refer to the gradual maturity of the pelvic bone structure as the Risser sign. The Risser staging system in the United States measures four stages (1 – 4) while the Risser staging system in France measures five stages (1 – 5). These measurements play an important role in how to treat adolescent idiopathic scoliosis and are referred to in different sample sizes in the white paper conducted by the Journal of Clinical Medicine.
The Tanner Staging System: Dr. James Tanner was a British pediatrician who in 1969 established a staging system for girls as they progressed through puberty. This staging system can be also referred to as Sexual Maturity Rating or better known as SMR. The Tanner grade is measured in five stages (1 – 5) and shows various stages of development in boys and girls. As per treating scoliosis the Tanner grade can make a difference in how doctors and therapists treat AIS (adolescent idiopathic scoliosis).
Why Was The Study On Bracing in Adolescent Idiopathic Scoliosis Done?
To get a glimpse into what is the objective of the study, we first need to understand the inspiration for the aggregation of such detailed research on scoliosis bracing. Any parent whose child has scoliosis understands the challenging lifestyle that the condition brings with it. Besides the pain increasing with further progression of scoliosis of the spine, there are negative social elements as well. Scoliosis patients tend to find it hard to fit into the proper clothing due to having uneven shoulders and will often cover up to show less flesh during the hot summer months. This can negatively impact their social life which can in turn be detrimental to friendships and establishing more meaningful relationships.
What if there was a non-invasive solution to treat and correct adolescent idiopathic scoliosis? That’s where scoliosis bracing comes into conversation. Ever since the origination of the creation of the Lyons Brace in 1948, doctors and therapists have been trying to develop a non-invasive approach for treating scoliosis. But the question always remained if bracing therapy is effective enough to alter an adolescent’s lifestyle by having them wear a brace full time. Though brace creators like Dr. Jacques Cheneau of France, and Dr. Emanuel Rigo of Barcelona, Spain have tried to make a light, fitted, and more comfortable brace, still no one said wearing an orthopedic device is easy. In addition, most brace therapies require the brace to be worn around the clock.
This is why the Department of Orthopaedic Surgery in conjunction with the University Medical Center Utrecht, both residing in The Netherlands, grouped a research team to investigate how effective scoliosis brace therapy is. The findings would help justify brace therapy for treating adolescent idiopathic scoliosis.
What Were The Findings In The Study?
To give the findings credibility, a variety of scoliosis braces were chosen for the study most of which were rigid and were worn full time. There was one brace called the SpineCor Soft Brace, which was soft but was still worn full time. The Charleston and Providence braces were the only night time braces worn in the study group. Researchers wanted to get a bird’s eye view from general bracing therapy for scoliosis and were not biased towards any particular brace.
When an orthotist wants to determine if the brace therapy regimen was successful they will look at the progression of the spinal curvature. In general, the ideal treatment plan for scoliosis would result in a normal Cobb angle of 10° or lower. In the study, success was defined as ≤5° curve progression during the follow-up visit after brace therapy. Therefore, if a patient started out at a 20° scoliosis curve and treatment brought it down to 15°, the study would call that a success.
The study population varied between 23 to 843 patients in which multiple bracing devices were used in each study. Every patient kept to the specific brace given to them throughout the treatment period. The Boston brace, which was used in three studies in a total of 169 patients, saw an average of a 67% success rate (53% – 83%). In another four studies, the Rigo-Chêneau brace was used and saw a success rate of 80% and was most effective in lumbar curves. The Progressive Action Short Brace (PASB) was used in two separate studies of 69 and 163 patients and saw a success rate between 65.6% and 100%. Similarly, the Lyon brace was used in 69 patients and reported a success rate of 99%.
Conclusion
The commonality between all of the brace therapy treatments for patients was that it was indeed an effective method of treatment for scoliosis. The rigid braces were more effective then the soft brace, and as you guessed it, full time wearing was more effective than part time wearing. Other important findings included brace therapy for scoliosis in Risser stages 0 – 2 and 0 – 3 of bone maturity appeared to be most effective. As the staging for skeletal maturity increases the effectiveness for scoliosis bracing therapy decreases. This is why it’s important that patients with adolescent idiopathic scoliosis get seen sooner rather than later in order that bracing therapy remains on the table as an option for treatment.

Another interesting finding in one of the studies was that when comparing the TLSO brace (thoraco-lumbo-sacral orthosis) to the Rigo-Chêneau brace, no patients of the Rigo-Chêneau brace required scoliosis surgery as opposed to 34% of TLSO brace patients required scoliosis surgery. This is one of the only findings that sided with one brace over the others in the comparative analysis. From there it appears that the Rigo-Chêneau brace is a highly effective method of bracing therapy for treating scoliosis and to avoid surgery.
Final Words
Whether or not you decide to seek brace therapy for your child is a conversation that should be between you, your pediatrician, and your child. Choosing to treat scoliosis with a brace will mean your child adhering to the prescribed treatment regimen for it to be most effective. After reviewing the study on The Effectiveness of Different Concepts of Bracing in Adolescent Idiopathic Scoliosis, it is clear that a full time treatment regimen is more efficient for treating scoliosis. With bracing therapy comes wearing the brace all throughout the day with short breaks for bathing. Though it’s tough to get used to at first, most adolescents will get used to it within a couple of weeks. Perhaps treatment will be complete within a twelve month period or sooner based on the time it takes to correct the spinal curvature. With all the discomfort that a patients endures during this period, it is they who are the true heroes. No surgery and normal spinal curvature, and that’s a win win for all. If your child has scoliosis, do a little research into bracing therapy and see if it’s right for them. As per this type of scoliosis therapy, a little discomfort can be truly a life changer. Good Luck!