
What To Do If Scoliosis Surgery is Recommended For Your Child
“How’s your granddaughter feeling?” I inquired from my close friend Brenda when meeting her on the avenue. “The operation went well but after two weeks she is still in a lot of pain. My daughter, her mom, is trying to keep her pain tolerable with Motrin but she ends up having to go back to the stronger prescription that was given to her originally in the hospital post-operative.”

It’s such a struggle to come to terms with a diagnosis that your child will need surgery for correcting a severe scoliosis condition. Another example of a teen who underwent scoliosis surgery recently was a close relative of mine and her mother claimed that the operation was quite successful, and I am certainly a witness to the acute transformation from a slouchy kid to a teen who looks a couple of inches taller. When I asked her mom if there were any side effects from her surgery she answered, “Just one, she can’t bend her back”. Now we know that squatting is much healthier for the back than bending but practically speaking, this limitation can have great ramifications for a girl just beginning high school. Gym and sports are enjoyable pastimes and classes and I wonder how she is managing her restriction.
Most scoliosis surgeons believe that only a minute number of severe scoliosis conditions are dangerous from a life-threatening point of view. Included in this view are children under the age of five who have inborn spinal curves that would affect the performance of the heart and lungs. When the lungs are not fully developed there is a slight danger that a severe scoliosis curve could cause the heart to stop beating. However, most surgeons are in agreement that past the age of five, it is not life- threatening except in extraordinary situations.
Often, teenagers are put to surgery prematurely when their scoliosis curve measures over 50 degrees or when the child stops growing. When a doctor says, “surgery must be done immediately” does this announcement leave no other option? Let us explore the facts, benefits and risks of spinal surgery to correct scoliosis.
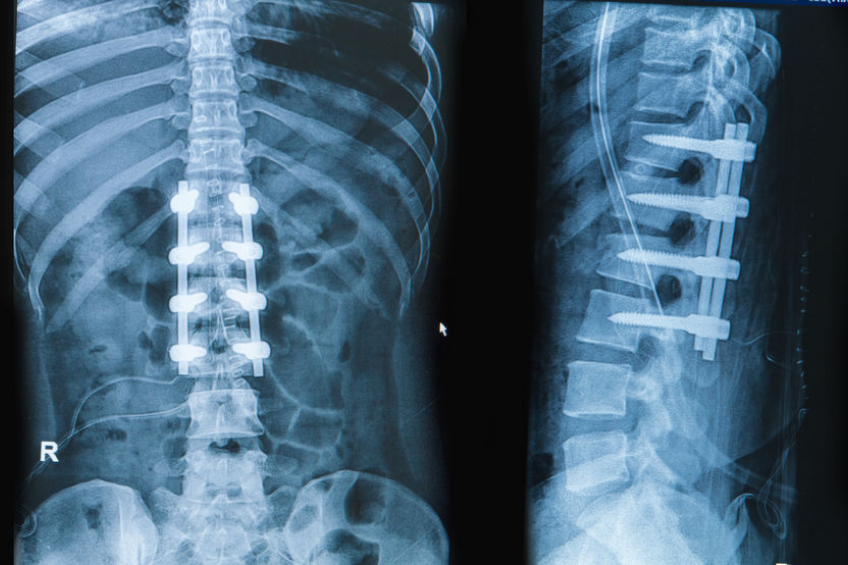
There are generally two types of scoliosis surgeries which are being used and have been used in the past. The first, posterior (patient lying face down) is when the patient’s curvature involves the upper thoracic spine. The second type of surgery is anterior surgery which involves a cut that follows the bottom ribs ending in an up-down direction above the navel which accesses the lower spine in an easier manner.
Another newer method of surgery that has been recently developed called Tethering uses “growing rods”. Other recent advances include fusionless procedures such as VEPTR – vertical expandable prosthetic titanium ribs (Invented by Dr. Robert Cambell of Children’s Hospital of Philadelphia). This system uses a curved metal rod that is surgically attached to a child’s spine or ribs hooked up on both ends of the device. This method is usually used to treat a congenital condition that prevents normal lung development).
Another novel technique, vertebral body spinal stapling, is a possible alternative to bracing for patients who are at risk for a speedy progression of the curve, and who may need a spinal fusion in the future.
One Person Who Defied the Odds
Meaghan Duggan was diagnosed with major advanced double curve idiopathic scoliosis when she was fourteen years of age. Meaghan was put into a brace immediately. Meaghan learned that 90% of patients with as severe a curve as hers need a spinal fusion operation. Being in a lot of pain along with the normal pressures of teenage life turned her into a real fighter. Keeping herself braced for twenty-three hours of the day, Meaghan defied all odds and her stats changed remarkably and there is essentially no probability that she will ever need surgery. Meaghan beat the odds and she is now giving other girls with her condition the strength and confidence to work hard and show the world that there is an alternative.
Meaghan must have amazing parents who did not listen to the experts and tried bracing and won. There must be lots of determination to beat the odds when you are in pain both physically and emotionally.
A Surgery Survivor
When beautiful Katie Fitzpatrick, was eleven years old she was examined for scoliosis at an annual school checkup as required at that age. After rechecking her back a few days later, the nurse sent Katie home with a letter for her parents with Katie trembling with fear that something was terribly wrong with her. When her parents finally revealed to her that she probably suffered from scoliosis, Katie then noticed that night that her shoulder blades and hips were uneven. Wow was Katie upset!
At an appointment at the pediatrician a few days later, Katie was informed that she did have a curvature of the spine and only x rays could determine the severity of the curve. A specialist at Children’s Hospital in Philadelphia informed her a week later after reading her scans that she was a candidate for surgery and at this point bracing was not an option!
Although Katie’s curvature was about 43% (much less than Meaghan’s) she was not given the option of bracing. Dr. Amar Samdani of Shriners Hospital for Children in Philadelphia was chosen as her surgeon.
The Tether-Vertebral Body Tethering Surgery
Dr. Samdani prescribed Verbal Body Tethering (VBT), at the time, (2014) an experimental procedure that had the distinct advantage of leaving the patient with almost total flexibility.
In the past if bracing did not work the next step was spinal fusion surgery. Metal rods are implanted along either side of the spine to correct the curve. Although spinal fusion is a good choice, patients find that tethering maintains the natural motion of the spine optimally.
By using the patient’s own growth process, the Tether straightens the spine. This is called “growth modulation”. The tether has the exclusivity of being the only process that treats scoliosis while the child is still growing and the growth itself is what repairs the curve. It’s sort of like an “internal” brace for your spine. As opposed to spinal fusion, tethering uses no metal rods. Katie was young enough to take advantage of this surgical method since she was still growing.
Katie’s Recovery From Surgery
Although Tethering sounded like an amazing improvement over spinal fusion, Katie’s recovery was far from uneventful. Leaving the hospital after five days, Katie needed to be homeschooled since she could not do much physically. After six weeks she was practically 100% recovered and was able to go back to school and partake in all school activities including her favorites volleyball and swimming.
Wait! Katie’s challenges were not quite over. In fact, the worst was yet to come. Six months after her first surgery, Katie was informed that she needed additional surgery to correct spondylolisthesis (slip-disk). Although they knew before her first surgery about this second condition, the doctor did not think she would need correctional surgery for the slip-disk. The second surgery was a mini fusion in the lumbar section of the spine.

Two months later, Katie’s second surgery was performed and the recovery from this surgery was much harder than the first. Our heroine had to endure both types of surgery within a year, Tethering and spinal fusion, nevertheless, Katie recuperated completely and was able to return to school the following year.
The Harm Study Group
The treatment of Idiopathic Scoliosis is a constantly changing field. Therefore, Professor Jeurgen Harms, a spinal deformities surgeon came up with the idea of having the most trusted surgeons pool their resources and knowledge to help each other and their patients. In 2011, a handbook was published titled, Adolescent Idiopathic Scoliosis which was translated into several foreign languages presenting completely unbiased research in the field. Dr. Peter Newton, one of the physicians in the group says that their goal is find a cure for scoliosis and the be a think tank for professionals to share their different medical strategies.
Final Words
We have attempted to give you a glimpse into the complicated world of scoliosis surgery. Surgery for scoliosis is not a medical emergency the same way that a ruptured appendix must be dealt with. If your child has a serious cobb spine curvature and surgery is recommended you should try to avoid it if possible. Sometimes trying even harder with physical therapy and more serious bracing might be the difference between surgery or not. Unless your child is suffering from a severe spinal deformation from birth that affects their breathing and heart, please check out more than one orthopedic doctor who specializes in Idiopathic Scoliosis.
If surgery is a must check out the new options available that are either less evasive or less risky such as Tethering, VEPTR and vertebral body spinal stapling. Organizations such as the Harm Study Group which is associated with the Clear Institute are knowledgeable on the latest possible advances on bracing and surgery for Idiopathic Scoliosis. Even if your child’s back is seriously curved, he/she can still beat the odds as Meaghan Duggan did.